![]()
Caesarean
section in a female rabbit having a difficult delivery
Esther van Praag, Ph.D.
|
MediRabbit.com is funded solely by the
generosity of donors.
Every donation, no matter what
the size, is appreciated and will aid in the continuing research of medical care
and health of rabbits.
Thank you
|

Warning: this file
contains pictures that may be distressing for people.
|
Pregnant
females rarely present a problem unless they are exposed to a stressful
environment, present abnormal deformations of the reproductive tract, or have
only one large fetus. This can lead to complications like toxemia or
anorexia. The
presence and the number of developing fetuses can be established around the
10th day of gestation. At this period of time, they form small grape-sized
masses in the ventral abdomen. At a later time, it becomes difficult to
differentiate the fetuses from the surrounding intestine and other organs. The
gestation period lasts between 29 and 32 days, exceptionally 35 days.
Parturition is rapid and, in most cases, lasts no longer than 30 minutes.
Natural abortion is rare in rabbits and is only observed after the 24th day
of gestation. Exceptionally, the interval of time of delivery between one
fetus and the next exceeds over an hour and the female is found straining and
exhausted. Medical assistance is needed at this stage. Caesarian
section procedure
The
presence of retained fetuses can be determined by palpation, ultrasound or
X-ray. If no
physical obstruction is diagnosed, the delivery can be activated by
administration of calcium and oxytocin (1-2 IU/kg, IV, IM). If a blockage or
narrowing of the birth passage, an abnormal size of the fetus, shape, or
positioning in the reproductive tract (dystocia) or uterine inertia is
diagnosed, caesarean section is the sole life-saving option for the doe and
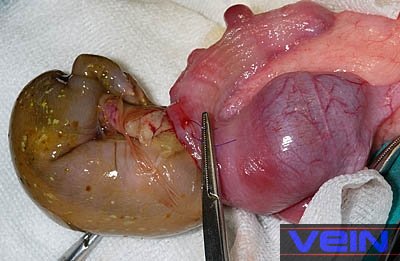
its newborn. The
procedure is uncomplicated, but needs to be done fast, to avoid asphyxia of
the fetus(es). The female
rabbit is placed in dorsal recumbency, with the
head slightly elevated. A surgical midline incision is made into the
abdominal cavity (laparotomy). The gravid uterus can be easily located and
can be quickly exteriorized in order to take out the fetus(es). Recovery
of the doe is generally uneventful. To
avoid future problems of unwanted litter and health problems for the doe, an
ovariohysterectomy surgery is recommended. This surgical procedure is done
under general anesthesia, in a sterile environment, with sterile surgical
instruments and a preparation of the skin. Indeed, any post-surgical
infection becomes a medical emergency. For more
detail of the spay surgery: ”Female reproductive tract and ovariohysterectomy” Pictorial midline caesarian section
Post-surgical
care
The administration of oxytocin (1-2 IU/kg, IM, IV)
can help stimulate milk production. Administration of analgesics like e.g.
buprenorphine, followed by meloxicam, is necessary during several days
following the surgical procedure. Pain indeed induces stress and
physiological responses, which slow down the activity of the digestive tract,
delay food intake and recovery. The presence of blood in the urine during 24 to 48 h
post-surgery is sometimes observed. Acknowledgement
Many thanks to Akira Yamanouchi (Veterinary
Exotic Information Network, Japan) and Karen Comish
(Israel) for the permission to use their pictures to illustrate this page. Further
Information
Harris WH, Yamashiro S, Stopps
TP. The effects of cesarean section anesthesia on heat loss and heat
production in the newborn rabbit. Can J Comp Med. 1983; 47(1):79-83. Morgan DR. Routine birth induction in rabbits using
oxytocin. Lab Anim. 1974; 8(2):127-30.
Jenkins JR. Surgical sterilization in small mammals.
Spay and castration. Veterinary Clin North Am Exot Anim Pract.
2000; 3(3):617-27. Millis DL, Walshaw R. Elective castrations and ovariohysterectomies
in pet rabbits. J. Am. Anim Hosp. Assoc. 1992:
491-497 Quesenberry KE, Carepenter JW, Quesenberry P. Ferrets,
Rabbits and Rodents: Clinical Medicine and Surgery Includes Sugar Gliders and
Hedgehogs, Elsevier
Health, 2004. Harcourt-Brown F. Textbook of
Rabbit Medicine, UK: Butterworth-Heinemann, 2001. Flecknell P ,
editor. BSAVA Manual of Rabbit Medicine and Surgery, Gloucester, UK: British
Small Animal Veterinary Association, 2000.. |












e-mail: info@medirabbit.com
