![]()
Nephroliths and uroliths (calculi) in rabbits
Esther van Praag, Ph.D.
|
MediRabbit.com is funded solely by the
generosity of donors.
Every donation, no matter what
the size, is appreciated and will aid in the continuing research of medical care
and health of rabbits.
Thank you
|

Warning: this file
contains pictures that may be distressing for people.
|
Nephroliths and uroliths, also called kidney and bladder calculi or
stones, are regularly seen in rabbits, independently from age and breed. Male
rabbits are more prone to the development of stones, due to their long
urethra. These stones are rock-hard crystal aggregations that exist in a
range of shapes and sizes. When they are small, but present in large
quantity, the condition is referred to as “sludge” or “sand”.
The basic mineral components of urinary calculi are
usually struvite (magnesium, ammonium, or phosphate), oxalate, carbonate,
uric acid, urate, or cystine. In rabbits, they are
commonly composed of calcium carbonate or oxalate dehydrate.
The presence of sand (sludge) or urinary
calculi is irritating to surrounding tissues and will lead to damages such as
kidney failure or the appearance of mucosal hemorrhages on the bladder wall.
As a consequence, there is bleeding and appearance of (microscopic) hematuria
(presence of blood in the urine). Smaller stones pose an additional danger as
their presence can lead to the obstruction of one or both kidneys. Once in
the ureter, they cause obstructions; the urine flow will be partially or
totally blocked and the rabbit will not be able to urinate. This will lead to
irreversible damage of the kidney and death if left untreated.
The exact cause leading to the formation
of bladder or kidney stones is unknown, but a variety of predisposing factors
are known to play a role. They include: Physiological causes: •
a genetic predisposition, that affect the
functioning of the kidney; • presence of bacteria in the bladder; • a kidney disease that influence the
excretion of calcium; • a bladder disease, with a modification of
the lining of the wall, due to the presence of pathogen bacteria or neoplasia
(tumor, polyps), • obesity, arthritis, leading to urine
retention due to reduced visits to the litterbox; •
change of the pH of the urine. Husbandry
causes: •
reduced water intake, due to a difficulty to drink
from a bottle, a defective water bottle, overturned crock, lack of fresh
water, or addition of medication in the drinking water; • improper litter possibilities, due to an
unclean litter-box, or one place in a wrong location; • calcium supplementation; •
Vitamin B6 deficiency, leads to increase
formation and excretion of oxalates. High urine pH
The urine
pH in rabbits is naturally high, between 7.6 and 8.8; with a specific gravity
is around 1.030. The latter is difficult to measure due to the presence of
calcium and crystals (struvite, calcium carbonate, more rarely oxalate). A high
pH favors the development of bacteria and UTI. Most commonly found bacteria
are Escherichia coli, Proteus sp. and Staphylococcus
sp., sometimes true-anaerobic bacteria are found. The bacteria will start to excrete
waste (ammonium) and an enzyme, urease that will break down the urea. The
high pH will accelerate the precipitation of struvite crystal. The presence of bacteria can be checked
by sending a sample of urine for bacterial culture (urine is normally sterile).
An alternative is to keep the removed uroliths,
open it, and use the central part for bacterial culture or have the stone
examined for the crystals composition. Indeed, some bacteria are associated
with a particular type (e.g. Staphylococcus sp. is associated to
struvite calculi).
Calcium in the diet
The
calcium content of the diet is often pointed as a cause for nephro- and uroliths in
rabbits. While the equation ”more calcium intake =
more calcium excretion” is true, it has been shown that feeding a high calcium
diet to rabbits resulted in the calcification of the kidneys (and the aorta),
the excretion of the excessive calcium via the urine, and not in the
formation of stones. It was, however, found that a short-time obstruction of
the urinary ducts would inexorably lead to the formation of stones. Causes
for such obstruction can be sludge, presence of a bacterial infection, an
abscess or neoplasia (e.g. tumor, presence of polyps). The
calcium content of the diet is not the primary factor leading to the formation
of stones in rabbits – rather a contributing factor – and it is important to
look for the main cause or underlying diseases. In an attempt to reduce the calcium
intake, it is sometimes advised to feed a low-calcium diet and/or stop
feeding pellets. This is not advisable. Indeed, rabbit have teeth that are growing
continuously, and thus need a daily minimal supply of calcium through their
diet. A diet low in
calcium or devoid of pellets can lead to mineral and nutrient deficiencies. Clinical signs
A rabbit
suffering from stones is often in pain. As a result, its appetite is
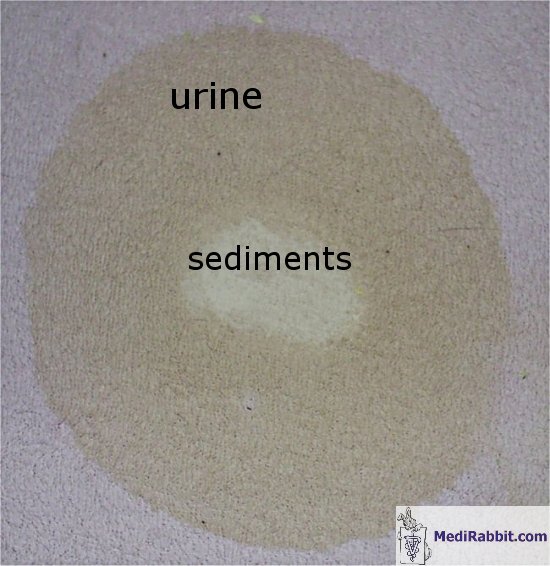
decreased, it is depressed and it may whine when urinating. Often, frequent and long urination is
observed, accompanied by urine dribbling. In some cases, the urine is so rich
in sediments (calcium carbonate) that the urine takes a paste-like
consistency, and stains the perianal region. Hematuria
is commonly seen. The amount of blood ranges between: •
microscopic amount, that can only be determined with
help of a dip-stick or by microscopy, •
large amounts of blood that color the urine in red or
brown. The later condition must be differentiated from the presence of
porphyrin, a plant pigment that naturally colors the urine in orange or red. NOTE: in female rabbits, the origin of the blood
in the urine must be determined, in order to rule out a uterine disease. In
the later, the blood appears only at the end of the urination process,
forming a stain in the middle of the urine puddle. This is a serious condition, which requires
urgent treatment. Diagnosis
The
presence of stones may be detected by palpating the bladder, which located in
the caudoventral abdomen. This must, however, be
done with care, in a co-operative rabbit only. More
reliable and precise diagnostics tools are X-ray and ultrasonography. A KUB (Kidney, Ureter, Bladder) X-ray
picture will reveal all calcium based stones larger than 2 mm. Uric acid
stones are not detected by X-ray, but those are exceptionally seen in
rabbits. The X-ray picture will help determine the size, the location and the
number of stones present. It is indeed important to verify the presence of
stones in the kidney, the urinary ducts (urethra and ureter) and in the
bladder, before starting their surgical removal.
It is
advisable to accompany the X-ray examination of the urinary tract by
ultrasonography (ultrasound examination), as it can detects
stones of 1 to 2 mm of diameter, than remain unseen on X-ray. Beside stones,
it enables to get a picture of the bladder wall, the kidney tissues, and can
show the presence of a blockage inside the kidneys or the ureters.
Exceptionally,
CT scans can be made, when an obstruction is suspected. It may furthermore
reveal further non-stone related problems, which may be mimicking the same
symptoms or discomfort. Last, but not least, an accompanying urine
and complete blood panel analysis, including serum biochemistry, will help
determine the general health condition of the rabbit, more particularly the
functioning of the liver and the kidney. Treatment
Depending on the size of the calculi,
several treatment options are possible. When
sand is present in the bladder, catherisation and
flushing brings good results. Indeed, manual expression of the bladder is not
recommended, as this organ can easily be ruptured, all the more in presence
of a small calculus that can block the urethra. The placement of a urinary
catheter (e.g. 5 French polypropylene or rubber catheter) is relatively easy
in male rabbits and requires only an injection of butorphanol
tartrate and the application of lidocaine on the prepuce (fold of skin near
the tip of the penis). Female rabbits often require a full anesthesia to
place the catheter. The female rabbit is placed in ventral recumbence, with
the rear limbs hanging off the edge of the table. The catheter is gently
introduced (blind guide) and its placement is confirmed by X-ray. Another
approach is to anesthetize the rabbit and administrate diazepam to relax the
sphincter, before placing the catheter. The
bladder is carefully flushed with a lukewarm saline solution, after which the
solution is removed with a syringe. Alkaline chemical solution that can
dissolve urinary calculi are used (acidic solutions lead to bladder and
urethra damage). The process is repeated several times. In
case the rabbit cannot be anesthetized, the alternative consists of massive
administration of fluids (within safe range), followed by the administration
of a diuretic drug (e.g. furosemide). This can be repeated over a few days,
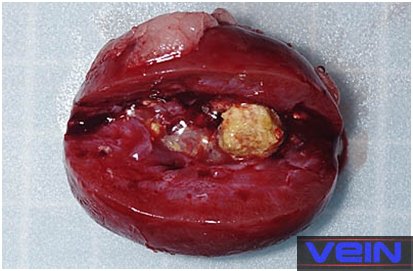
each time in well-hydrated rabbits. Surgery remains the sole option when the
urinary calculi are large. After induction of anesthesia, the bladder with be
exteriorized and opened. After removal of the stone, it is advisable to take
a sample of the bladder wall, for bacterial culture.
Post-surgical
care includes pain medication, antibiotic therapy when necessary, and the
analysis of the underlying cause leading to the formation of urinary calculi
or sludge. Long-term
management includes increase of water intake by the rabbit, for example the
administration of subcutaneous fluids once every day or every second day
(e.g., 50 ml). This will help flush
his kidney and bladder and avoid the accumulation of compounds prone to start
a stone. Various
products can furthermore be given to the rabbit in order to decrease slightly
the pH of the rabbit. They include: • Feeding fresh or dried cranberry daily or
non-sweetened cranberry juice. • Vitamin C. For smaller animals,
the intake of Vit C is up to 100 mg, probably best
between 25-50 mg/kg rabbit once a day. Part of the Vit
C will be converted in oxalates, which may start a stone, but studies showed
that high intake of Vit C did not contribute to the
formation of stones. The subject remains
a bit controversial among professionals. • Use of citrate based products
(e.g. Polycitra®) in order to change the pH of the
urine, in rabbits that suffer from chronic urinary tract infection or uroliths (bladder stones). The daily dosage in dogs is:
150 mg/kg per day. It has been used in rabbits and seems to have delayed the
formation of new stones. It should be kept in mind that long-term urine
acidification of the urine is harmful to the rabbit. • Use of acidifiers like ammonium
chloride (200 mg/kg/day, PO, TID) and DL-methionine (1,000-1,500
mg/cat/day, PO) may help acidify the urine. It should be kept in mind that
long-term urine acidification of the urine is harmful to the rabbit. • Addition of liquid magnesium into
the drinking water of a rabbit. One rabbit that has suffered from sludgy
urine during 6 years, and bladder flushing every 6 to 12 months. Since he
started this treatment, there is no sludge anymore. It is not so much the product that is
important, but the fact that the urine is acidified. This acidification
dissolves the magnesium-ammonium-phosphates stones or prevents their
formation.
Acknowledgement
My gratitude goes to Dr Christiane Nastarowitz-Bien
(Germany) pour her help and suggestions. A great thank you also to Christine Macey (USA), Hilde Seep (The
Netherlands), Prof. Ruby L. Perry (College of Veterinary Medicine, Michigan
State University, USA), to Andrea Pons (Allemagne, Kaninchenforum.com), to
Sebastian P. (Croatia) and to Akira Yamanouchi (Veterinary Exotic Information
Network, https://vein.ne.jp/, Japan), for the permission to use their pictures. Further Information
Donmez T, Erol K, Gurer
F, Baycu C, Acikalin E, Cingi MI. Effects of various
acidic and alkaline solutions used to dissolve urinary calculi on the rabbit urothelium. Urol Int. 1990;
45(5):293-7 Hanke PR, Timm P, Falk G, Kramer W. Behavior of different suture
materials in the urinary bladder of the rabbit with special reference to
wound healing, epithelization and crystallization. Urol
Int. 1994; 52(1):26-33. Garibaldi
BA, Fox JG, Otto G, Murphy JC, Pecquet-Goad ME.
Hematuria in rabbits. Lab Anim Sci. 1987 Dec;37(6):769-72. Erratum in: Lab Anim
Sci 1988; 38(3):345. Garibaldi
BA, Goad ME. Hypercalcemia with secondary nephrolithiasis in a rabbit. Lab Anim Sci. 1988; 38(3):331-3. Itananin et al. Experimental
model of calcium containing renal stone formation in a rabbit. Invest. Urol. 1979;
17:234-241 Kamphues J., Carstensen
P., Schroeder D., Meyer H., Schoon H.A., Rosenbruch M., 1986. Effects
of increasing calcium and vitamin D supply on calcium metabolism of rabbits. J. Anim. Physiol. a. Anim. Nutr.,
56, 191-208. Kamphues J. Calcium metabolism
of rabbits as an etiological factor for urolithiasis. J Nutr.
1991;121(11 Suppl):S95-6. Lee
KJ, Johnson WD, Lang CM, Hartshorn RD. Hydronephrosis caused by urinary lithiasis
in a New Zealand white rabbit (Oryctolagus cuniculus).
Vet Pathol. 1978; 15(5):676-8. Whary MT, Peper RL. Calcium carbonate urolithiasis in a rabbit. Lab Anim Sci. 1994; 44(5):534-6.
White
RN. Management of calcium ureterolithiasis in a French
lop rabbit. J
Small Anim Pract. 2001;
42(12):595-8 |
|||||||||||||||||||||||||||||


















e-mail: info@medirabbit.com
