![]()
Schmorl’s disease or
skin necrosis due to
Fusobacterium necrophorum
Esther van
Praag, Ph.D.
|
|
MediRabbit.com is
funded solely by the generosity of donors. Every
donation, no matter what the size, is appreciated and will aid in the
continuing research of medical care and health of rabbits. Thank you |

|
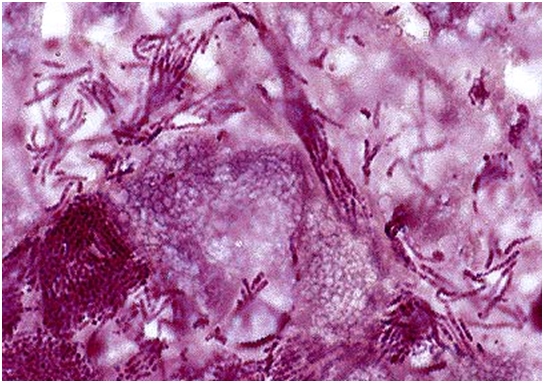
In 1891, the German pathologist C.G. Schmorl first
described the disease caused by the bacterium Streptothrix cuniculi.
It has been later renamed Fusobacterium necrophorum. Schmorl’s disease
affects animals, as well as man. Fusobacterium spp. is a non-motile, non-spore
forming, anaerobic, Gram-negative bacterium that belongs to the normal
intestinal bacterial flora of the rabbit. It is suspected that the disease is
spread by cecotropes. The lesions are indeed found mainly around the head,
the neck and the feet. This bacterium is also responsible for dental
disorders, like tooth root infections. The disease is associated to poor hygiene, and
husbandry, and is independent from the sex, the age or the breed of a rabbit.
Further sporadic causes for the disease are: • Ptyalism
due to dental problems, like malocclusion or tooth root problems; • Panting,
related to a environment with high temperatures or respiratory distress
(dyspnea); • Inappropriate
drinking tools, like a leaking water bottles, or an oversized dewlap getting
wet while drinking; • Cages
without rust and sharp edges.
Clinical signs and diagnosis The first
signs are an acute inflammation of the subcutaneous tissues. As the disease
progresses, there is ulceration of the superficial skin layer, suppuration of
the subcutaneous tissue and necrosis. In rare
cases, the disease is caused by Fusobacterium nucleatum in rabbits. The disease
is characterized by the formation of skin ulcers and subcutaneous abscesses on the
head, neck and feet. In rare cases, encapsulation of the abscesses by fibrous
tissue is observed. If the wounds remain untreated, the infection spread to
the skin, leading to necrosis of the tissue. The wounds can spread into
deeper tissue layer and cause osteomyelitis or septicemia, leading to
infection of vital organs and general toxemia. The rabbit is feverish and its
lesions spread a foul smell. In some cases, the rabbits suffer
a chronic attack of Fusobacterium sp. They show mainly a decreased
appetite (anorexia) and chronic weakness (cachexia). Treatment
To confirm the diagnosis, a
sample should be collected from the affected area and cultured. Similar
lesions are indeed caused by various other bacteria, including Pasteurella
multocida, Staphylococcus aureus or Pseudomonas aeruginosa.
The fur around the lesions is
carefully clipped and wounds are cleaned with an antiseptic solution. The
treatment must be accompanied by parenteral administration of antibiotics
like penicillin, cephalosporin, chloramphenicol, tetracycline or
metronidazole. Due to its good penetration of the bone, cephalosporin’s is
the antibiotic of choice when the bone is affected. The abscesses and necrotic tissue
must be excised surgically. If surgery is not possible, the
abscess cavity can be incised, drained and packed with an antibiotic
impregnated dressing. Various methods are available: • Permanent placement of antibiotic
impregnated PMMA beads; • Temporary filling with antibiotic
impregnated haemostatic and bactericidal sterile compressed sponge. The
dressing must be changed daily or every 2nd day, to avoid necrosis of
surrounding tissues; • Temporary filling with wet-to-dry
hygroscopic and bactericidal sugar dressing (e.g. 50% dextrose, manuka or
clear sterilized (g-rayed)
honey). The dressing must be changed daily, to avoid necrosis of surrounding
tissues. The later filling presents the
advantage to remove the malodorous smell of ammonium and sulfur compounds due
to bacterial breakdown of serum or cell proteins. Infection by Fusobacterium
sp. is generally difficult to treat and tends to return as soon as the
antibiotic treatment is stopped. To minimize recurrence the causes should be
looked for and corrected.
Further informationCrociani F, Biavati B, Castagnoli P, Matteuzzi D. Anaerobic ureolytic bacteria from caecal content
and soft faeces of rabbit.
J Appl
Bacteriol. 1984; 57(1):83-88. Garibaldi BA,
Moyer C, Fox JG. Diagnostic exercise:
mandibular swelling in a rabbit. Lab Anim Sci. 1990; 40(1):77-78. Hofstad T,
Sveen K. Endotoxins of anaerobic gram-negative rods. Scand J Infect Dis Suppl. 1979; (19):42-45. Kanoe M, Toyoda Y, Shibata H, Nasu T. Fusobacterium
necrophorum haemolysin
stimulates motility of ileal longitudinal smooth
muscle of the guinea-pig. Fundam Clin Pharmacol. 1999; 13(5):547-554. Licois D.
Tyzzer's disease. Ann Rech Vet. 1986;17(4):363-386. Nakajima Y,
Ueda H, Takeuchi S, Fujimoto Y. The effects of Escherichia coli
endotoxin as a trigger for hepatic infection of rabbits with Fusobacterium
necrophorum. J Comp Pathol. 1987; 97(2):207-215. Ormerod D,
Koh K, Juarez RS, Edelstein MA, Rife LL, Finegold SM, Smith RE. Anaerobic bacterial endophthalmitis in the
rabbit. Invest Ophthalmol Vis Sci. 1986; 27(1):115-118. Seps SL,
Battles AH, Nguyen L, Wardrip CL, Li X. Oropharyngeal Necrobacillosis with
Septic Thrombophlebitis and Pulmonary Embolic Abscesses: Lemierre's Syndrome
in a New Zealand White Rabbit. Contemp Top Lab Anim Sci. 1999; 38(5):44-46. Tyrrell KL,
Citron DM, Jenkins JR, Goldstein EJ. Periodontal bacteria in rabbit
mandibular and maxillary abscesses. J Clin Microbiol. 2002;
40(3):1044-1047. Ward GS, Crumrine MH, Mattloch JR. Inflammatory exostosis
and abscessation associated with Fusobacterium nucleatum in a rabbit. Lab Anim Sci.
1981; 31(3):280-281. |

e-mail: info@medirabbit.com
