![]()
Abscess Management in Rabbits:
an Illustrated Guide
Christine Macey
and Esther van Praag, Ph.D.
|
MediRabbit.com is
funded solely by the generosity of donors.
Every
donation, no matter what the size, is appreciated and will aid in the continuing
research of medical care and health of rabbits.
Thank you
|

Warning: this file
contains pictures that may be distressing for people.
|
An abscess is a pocket of fluid
and pus, which results from an attack by pyogenic organism (e.g. bacterium)
followed by the destruction of cells. The pocket usually contains a
collection of pus, dead phagocytic white blood cells, necrotic cells, and
live or dead bacteria. As the quantity of pus increases, the pocket grows
larger and starts to wall off from the surrounding tissues and blood
circulation. This renders treatment difficult. If the abscess is left
untreated, it continues to grow. Tissue will rupture either inside the body
or on the surface of the skin. This stage is particularly painful and
dangerous, with the liberation of bacteria and their toxins in the blood
circulation. In most cases of abscess, the
rabbit has a history of pasteurellosis, though other bacteria like Staphylococcus
aureus, Streptococcus sp, Pseudomonas sp. or Fusiformis
sp. are no exceptions. They often result from a nasolacrimal or tooth
problem, surgery, or a foreign body such as a hay splinter in the gum. Options that are available to
treat abscesses in rabbit include: ·
Total surgical excision of the
abscess cavity, necrotic tissue, and the surrounding fibrous capsule. This
treatment can, however, not be done when several abscesses are present, or
when the bone is affected (e.g. osteomyelitis, jaw bone infection by a tooth
root). When surgical excision is not possible, the cavity
should be packed with an antibiotic impregnated dressing. Various types are available nowadays: ·
Permanent placement of antibiotic
impregnated PMMA beads, ·
Temporary filling with antibiotic
impregnated gelatin sponge (e.g. GelFoam®, Surgicel®). The dressing must be
changed daily or every 2nd day, to avoid necrosis of surrounding tissues.. ·
Temporary filling with wet-to-dry
hygroscopic and bactericidal sugar dressing (e.g. 50% dextrose, or manuka or
clear sterilized (g-rayed) honey). The dressing must
be changed daily, to avoid necrosis of surrounding tissues. The later filling presents the advantage to remove
the malodorous smell of ammonium and sulfur compounds due to bacterial
breakdown of serum or cell proteins. Due to its richness in sugars, honey has an
hygroscopic effect on the wound, preventing bacterial development. Honey will
furthermore acidify the wound, accelerating the healing process. The honey
should not be boiled, otherwise its bacteriostatic/bactericidal properties
are lost. When used in abscess treatment, success cannot be guaranteed by a
100%, still we were able to treat successfully some intractable abscesses in
horses. Advantages in using honey are that the product is cheap, non-toxic
and treatment can be continued over a longer period of time. The goal for abscess treatment is to cure the
infection. Most people are afraid to hurt their rabbits, but they tolerate a
lot and it is necessary to do a good job on wound care or the surgery will be
for naught. Here we present daily care related to management of
the jaw abscess of Buh-Bunny. Background, by Christine
Macey
Buh-Bunny had about 5 of jaw abscesses if I count
correctly. He is my 4th jaw abscess
rabbit and lived the longest with them (3 years), and oddly enough a sarcoma
and not the abscesses did him in at 9 years old.
Buh-Bunny's first jaw abscess was 3 years earlier
and ceftiofur beads were implanted.
The next day he had another abscess removed from another spot in his
jaw found on closing the day before, ceftiofur beads placed too. He was on penicillin injections for a week. Three months later another jaw
abscess, but the beads did not stay suspended after surgery, falling down
into his dewlap so I cannot call this a true bead failure. The vet who placed these beads assisted
Kerin Tyrrell with her rabbit mandibular and maxillary abscess study, so the
choice of drugs for the next bead placement was clindamycin. We both chose
not to culture because of the poor culture results Kerin had received from
this area's labs, knowing it would be a waste of time and money. Buh-Bunny stayed abscess free for
a year but required another facial surgery for a lump that was reported as a
benign fibroma on the histology.
Buh-Bunny then quit going out on the lawn where the cottontails roam
as this was a probable cause. Another jaw abscess a year later
and I had read enough testimonials from trusted individuals to know I wanted
to try bicillin. My initial vet did
not want to go this route so I went to my local vet. I used bicillin alone for maybe a few weeks
but saw no decrease in abscess size so decided on surgical removal and wound
irrigations to let it heal inside to out along with the bicillin. This was also successful for a year. So, now we are on his 5th jaw abscess and I went to
my alternate vet (my local vet was not available), a 3rd vet I use frequently
when my local vet is not around, and she said it was inoperable. I used bicillin and Buh-Bunny began to have
more and more trouble eating.
I was not going to put him through
more surgery but ended up taking him to my local vet for a second opinion,
and he said it was certainly operable, that it would buy him time but in all
likelihood this would kill him in the end, but the end might be a ways off. I
asked if he would close it up and not leave me with a huge open wound and he
said he would if it wasn't too dirty but I ended up getting a smallish deep
hole which made observing the state of the wound hard. I believe he was on both bicillin and
naxcel (ceftiofur) injections but that doesn't really matter, and I cultured
to which is another story, but did it more for academic reasons and curiosity
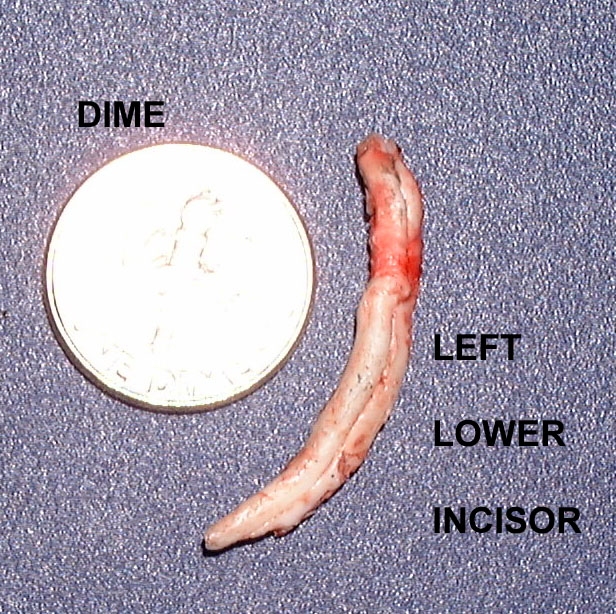
than for planning his drug therapy. Manuka honey is usually not the
first choice dressing for abscesses; it was the best selection given the
circumstances: a wound tract that exited through the cavity left by a lower
incisor removal, the entrance being on the outside of the left cheek. This
meant that anything I irrigated with would in part end up in my rabbit's
mouth. Summary of the procedure
used for dressing a wound with honey
1. Do not leave
it too late to start using honey on a wound. 2. Use only
honey that has been produced especially for use in wound care. 3. Use dressings
that will hold sufficient honey in place on a wound to get a good therapeutic
effect (i.e. about 20 ml/25 g per 10 cm X 10 cm). 4. Ensure that
honey is in full contact with the wound bed (i.e. fill any cavities or
depressions. 5. If a
non-adherent dressing is used between the honey dressing and the wound bed it
must be sufficiently porous to allow the active components of the honey to
diffuse through. 6. Ensure that
the honey dressings extend to cover any area of inflammation surrounding
wounds. 7. Use a
suitable secondary dressing to prevent leakage of honey. 8. Pressure
bandaging can be used over honey dressings. 9. Change the
honey dressings frequently enough to prevent the honey being washed away or
excessively diluted by wound exudate - if the honey gets washed away then the
dressings can stick and maceration of surrounding skin can occur. 10. When using
honey to debride hard eschar, scoring and softening the eschar by soaking
with saline will allow better penetration of the honey. Applying dressings
soaked in diluted honey (3 parts water or saline to honey) rather than
straight honey may give faster debriding of hard eschar. Procedure used for
dressing a wound with honey in pictures
EXTENT OF THE WOUND.
This shows the wound tract that had to be encouraged
to stay open long enough for systemic antibiotics to do their job and to
clean out any recurring infection in the wound bed. This also shows that a
bunny will tolerate a lot of manipulation of their wounds. I premedicate with
something like torbugesic 30 minutes before the procedure.
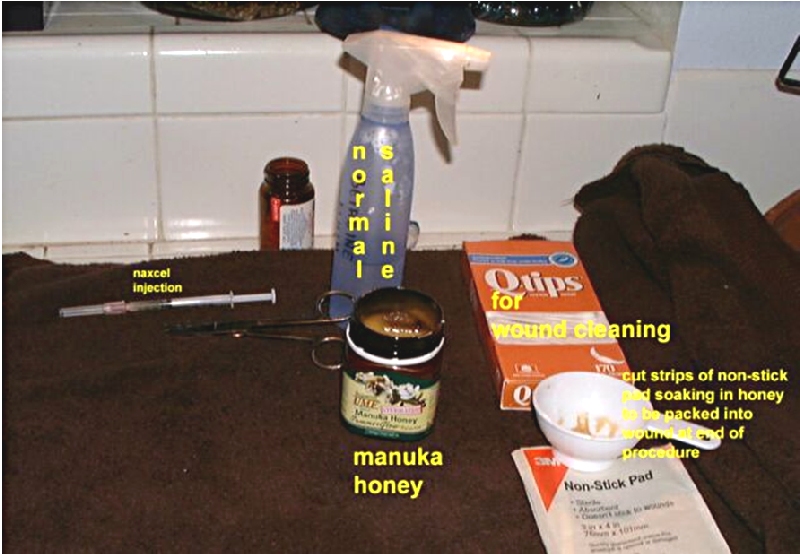
GETTING ORGANIZED BEFORE
STARTING.
This is very important. Have everything you will be
using at the ready. I've found that having a thick towel for the rabbit
footing makes him feel much more secure, and I prefer to do irrigations and
wound cleanings over the sink. The squirt bottle is by far the best tool in home
care irrigating. I started with a
Water Pik (about $80.00 in the States) and irrigating Froggie's jaw abscess
in the bathtub. The noise and weird
location probably added to her discomfort.
That was in 1997. By the time I
was irrigating Bupkiss' wound in '99, I used an 18-gauge catheter and 3 cc syringe. The squirt
bottle is cheap and works better; unfortunately it took me until 2002 to
learn that.
SALINE IRRIGATIONS.
After unpacking the wound I use a
squirt bottle and irrigate until I have a good flow from the entrance at the
cheek to the exit from the inside of his mouth, trying to keep him position
over the sink so the irrigant and debris does not get swallowed. This is when I would insert the Q Tip and use it as
a mechanical debridement and to open the wound back up. It is constantly
trying to close. This is also a
picture of a very clean wound.
Instilling
honey with 1 cc syringe.
I tried this method but learned right away that it
wouldn't work, this would not keep the honey in
contact with the wound bed. What I did was reread the directions (it's easy
to get overwhelmed in the face of having to do this) and cut up the
non-adherent pads into strips of gauze and soak them in honey/saline solution
per instructions. Then I packed the wound as best I could using hemostats or
tweezers to push it in.
Cleaned up and packed
wound.
Picture of a wound needing
attention. The white is not pus, much of it is dead tissue that needs to be
cleaned out as much as possible. Some is just debris that will wash away with
the irrigations. I learned a lot watching my vet clean a dirty wound. He
taught me that my rabbit would tolerate taking tweezers and pulling out dead
tissue. Dead tissue attracts bacteria. The purple is bruising that was evident in those
first post op days. There is also a
bit of dry gauze to seal the outside before the final dressing (as the final
dressing had a tendency to fall off a lot).
Happy
to be all done.
I used a product called Skin Prep which
has a skin protectant and makes the outer dressing stick better. Still, this
was often the way I'd find it in the morning:
Wound the next day.
He
would never pull the gauze out but the outside bandage would come off
frequently. Still, this is preferable to no packing at all and letting that
wound close right up. Keeping it open not only allows time for the systemic
antibiotics to do their job, but discourages anaerobic bacterial growth. I feel
the honey method would need to have more frequent dressing changes than our
usual twice a day cleanings and redressing with Buh-Bunny and for a variety
of reasons I didn't use honey to the end, but even so his wound was closing
up and I was at the stage where I'd let it win more and more until it is
finally closed. EVERYONE
NEEDS A FRIEND AFTER TREATMENT !!!
I would have loved to end with a picture
of a totally healed wound, but shortly after this Buh-Bunny died after
surgery to remove a large abdominal sarcoma. He passed quietly at home with
Keri by his side. I believe a treat or
comforting of some kind is due after this procedure. !! REMINDER !!
Always
take your bunny back to your vet when you are confused about the status of
the wound. There were times when I didn't know if I was looking at something
that should stay put or something that should come out. Acknowledgement
Thanks you oto Buh-Bunny and Christine Macey (USA). . |
||||||||||||||











e-mail: info@medirabbit.com
