![]()
Middle and inner ear (otitis
media and interna)
Esther
van Praag, Ph.D.
|
|
MediRabbit.com is
funded solely by the generosity of donors. Every
donation, no matter what the size, is appreciated and will aid in the
continuing research of medical care and health of rabbits. Thank you |

|
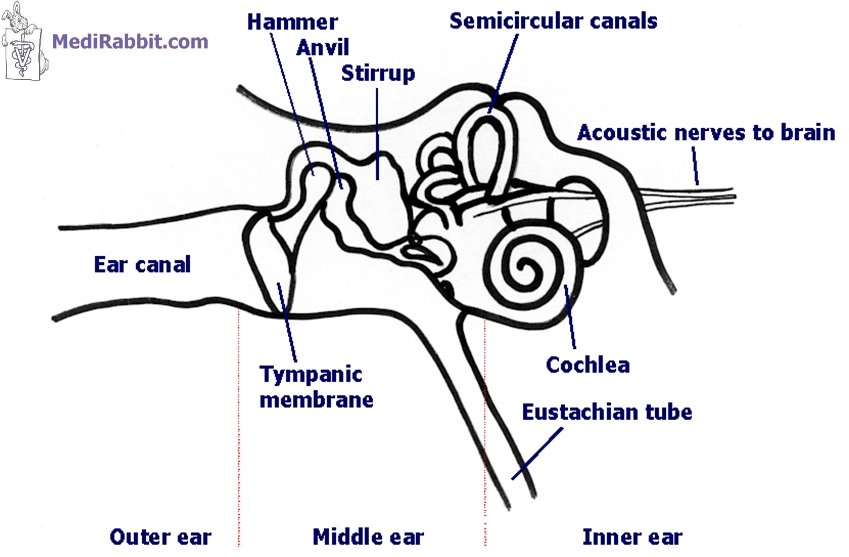
Otitis media and interna, Latin names for inflammation of the ear
chambers located behind the tympanic membrane (ear drum), involve
approximately 50% of all cases of acute vestibular disease. The middle ear is
the region located directly behind the tympanic membrane (eardrum). It is
composed of the various bones and nerves that facilitate sound diffusion from
the outer ear to the brain. The middle ear is connected to the nasal cavity
by the Eustachian tube, which enables the adjustment of the air pressure
inside the middle ear. It is responsible for maintaining equilibrium.
MediRabbit Mammalian inner ear Otitis
media, also known as a middle ear infection, is located behind the eardrum.
The presence of bacteria, fungi, yeast, or parasites can trigger the body's
natural response of producing fluid and pus. This process leads to
inflammation and pain, and in some cases, it may result in hearing loss.
In cases of
severe infection, there is a possibility of tympanic membrane rupture. The
pus contained in the middle ear will flow into the ear canal, and the
infection can spread to the outer ear. The infection can also spread from the
middle ear to the inner ear (otitis interna or labyrinthitis). The disease's
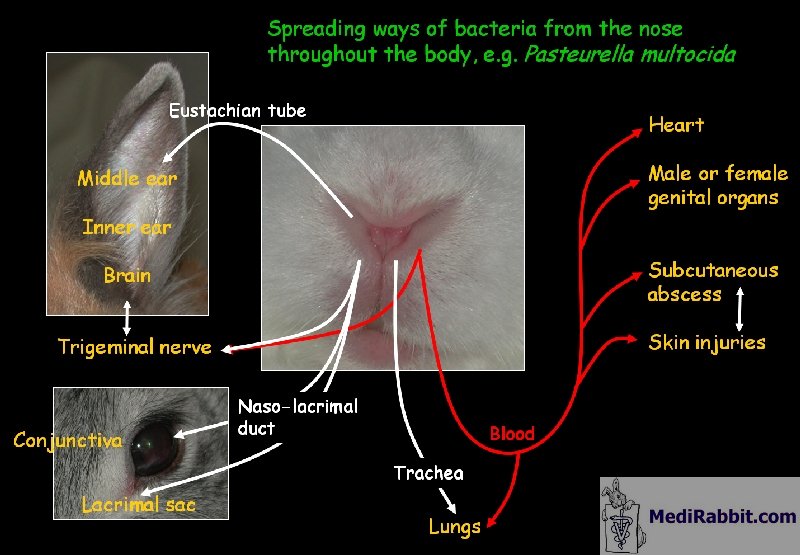
progression is characterized by head-tilt and ataxia (a lack of balance). Pasteurella multocida, a
natural host of the nasal cavity of rabbits is often associated with middle
and inner ear infection. It is important to note that healthy rabbits can
carry this bacterium without showing clinical signs. The progression of the
disease is influenced by the host's overall resistance and the virulence of
the Pasteurella sp. strain. It is believed that the bacterium migrates
from the nasal cavity to the middle ear along the Eustachian tube or
mandibular molar root abscess when there is exposure to the Eustachian tube. Staphylococcus aureus is
considered as an opportunistic pathogen of the nasopharyngal
cavity of rabbits. Its presence in the ear can lead to severe middle or inner
ear infection. The Staphylococcus aureus bacterium is known to
demonstrate resistance to one or more antibiotics. Further bacteria known to cause inner ear infection include Streptococcus
sp., Escherichia coli, Enterococcus sp, Proteus sp., Pseudomonas
sp.. Sporadic cases of yeast infection, e.g. Candida sp. or Pityrosporum
sp., are found in rabbits. Fungal infection, e.g. Cryptococcus sp., is
rare.
MediRabbit Spread pathways of bacteria from
the nasal cavity to the middle and inner ear Clinical
signs
Clinical signs for
otitis media can be absent. In many cases, the symptoms are similar to those of an external ear infection, including
shaking of the ears, scratching with paws, rubbing, anorexia, depression, and
pain. Discharge in the external ear canal is indicative of a ruptured
eardrum, resulting from internal pressure caused by infection. A middle ear
infection is typically accompanied by symptoms such as head shaking and
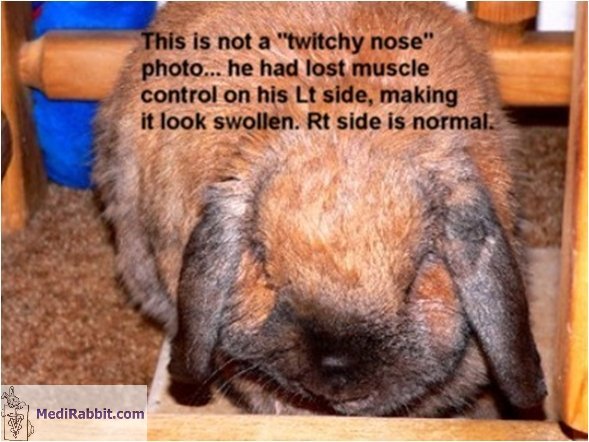
drooping of the ear. Facial paralysis may result from swelling and
compression of the facial nerve. Rabbits may experience hearing impairment
due to ear discharge in this portion of the ear. The condition is painful. Inner ear infection is characterized by
ataxia (circling, rolling, stumbling), a tendency to lean to one side, and a
head tilt. Some rabbits exhibit lateral head movements. This is due to the
pressure from infected tissue and surrounding inflammation, which causes the
compression of nerves passing through the vestibular region of the brain.
Kim Chilson Rabbit suffering
from facial paralysis: a front view from the face shows asymmetry of the
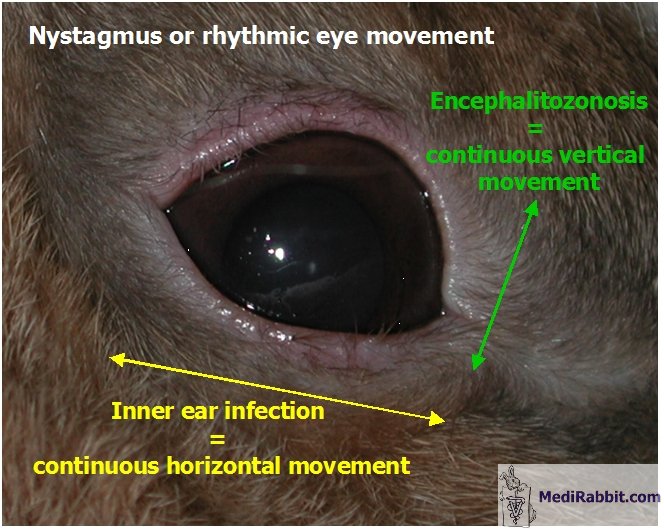
face. This is caused by the dropping of the lip on the paralyzed side The appearance of
nystagmus (involuntary rhythmic eye movement) is observed when treatment is
delayed or inappropriate. If observed, it may be indicative of an inner ear
infection or E. cuniculi. Depending on the location of the damage,
differences in eye movement are indeed observed: -
Bacterial
infection of the inner ear generally leads to peripheral vestibular disease.
This is characterized by horizontal and rotary nystagmus, but never vertical
nystagmus. -
E.
cuniculi is generally related to central
vestibular disease, which shows typically vertical and positional nystagmus,
more rarely horizontal nystagmus. The vertical nystagmus is the one mainly
observed in E. cuniculi suffering rabbits that do not suffer from
secondary inner ear infections. -
Rotary
nystagmus (in vertical and horizontal directions). This relates to lesions of
the cerebellum, the brainstem or the vestibular connections; causes can be
the presence of a tumor or a bacterial infection (encephalitis), to name the
main ones. The direction of repetitious involuntary eye
movement should not be a basis for a
final diagnosis
between the two disorders. Nystagmus is a clinical feature of various
diseases, including metabolic disorders, eye disorder (glaucoma, cataract,
retina problems, and albinism), nutritional deficiencies (e.g. magnesium,
thiamin, medication (e.g. barbiturates), the presence of brain lesions, or
trauma.
MediRabbit.com Middle ear infection may be accompanied
by continuous horizontal or rotary nystagmus, while nystagmus caused by E.
cuniculi is usually vertical, horizontal or positional
Renee Brennan Video of Rudy, a rabbit presenting clinical signs of encephalitozoonosis: severe involuntary head tilt and rhythmic horizontal movement of the eyes Diagnosis
It is important to differentiate ear infection from other causes of
vestibular diseases. See: Head tilt and their various causes. Otitis media is visible on X-rays, changes on
the level of the bullae, on the contrary of otitis interna and E.
cuniculi lesions. Changes of the soft tissue density are observed in the
middle ear, with appearance of an opaque grayish mass. It is sometimes
accompanied by sclerosis and bone proliferation, which may reach as far as
the temporal bone or the temporo-mandibular joint. X-ray can, furthermore,
help rule out dental problems or E. cuniculi.
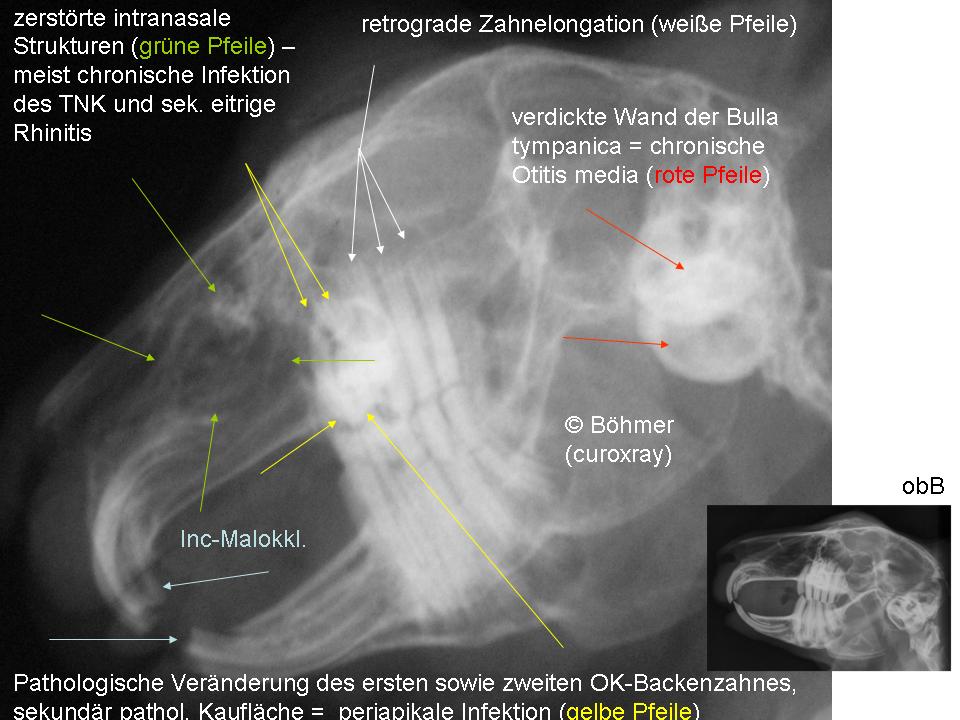
Dr. Estella Böhmer, curo–X-ray Chronic
middle ear infection can be seen on X-rays, with a thickening of the tympanic
wall (red arrows). This rabbit also suffers dental problems: malocclusion of
the incisors, retrograde elongation of the maxillary cheek teeth (white
arrows), a pathological modification of the first and second maxillary cheek
teeth and infection surrounding their roots (periapical infection - yellow
arrow). The x-ray also shows that the structure of the nasal cavity has been
destroyed (green arrow). This results often from chronic infection of the
nasolacrymal duct or secondary rhinitis accompanied by nasal secretions. If discharge is present in the outer ear, a culture should be
performed to determine if bacteria, yeast, or fungi are present. This should
be followed by a sensitivity culture to determine the most effective
antibiotic or antifungal treatment. Cytological methods are essential in the diagnosis of various medical
conditions. These methods allow for precise identification of bacteria,
yeast, and fungi, in addition to specific types of cancer. A complete blood count (CBC) and biochemistry panel can help determine
the presence of an infection or E. cuniculi, with neutrophilia or changes in
values related to kidney function (BUN, creatinine), respectively. Serological tests are used to determine exposure to E. cuniculi or
Pasteurella sp. during its life. A high titer is indicative of an active
infection by E. cuniculi. Treatment
The
antibiotic treatment plan should be based on the results of the sensitivity
culture. However, this is not always feasible. In such cases, the
administration of antibiotics known to cross the blood-brain barrier is
necessary. Chloramphenicol
and penicillin (bicillin) antibiotics have been
shown to successfully pass the blood-brain barrier and have been used to
treat middle or inner ear infection in rabbits. Trimethoprim sulfate is
occasionally recommended, but its efficacy in rabbits is reportedly
unsatisfactory. This could be related to the drug's half-life of
approximately 40 minutes in rabbits. Ciprofloxacin and marbofloxacin have
been successfully used to treat an inner ear infection in some rabbits. In
certain cases, the administration of combined antibiotic therapies is an
effective treatment option. Examples of such therapies include
enrofloxacin/chloramphenicol and marbofloxacin/penicillin. The treatment
plan must be both aggressive and prolonged, with a duration of at least four
to six weeks, or two additional weeks following the complete resolution of
symptoms. If no improvement is observed after 14 days, it is possible to
switch to another antibiotic. To minimize the appearance of resistance in the
pathogenic bacteria, it is recommended to administer a combination of the old
antibiotic and the new one. An otoscopic
examination is essential to determine if the eardrum has ruptured. If this is
the case, the use of antibiotic-containing eardrops may result in
ototoxicity. The consequences include permanent hearing loss, loss of
balance, or death. A safe alternative to remove pus and debris is to wash out
the outer and middle ear with a saline solution. The
antibiotic therapy should be accompanied by NSAIDs (non-steroidal
anti-inflammatory drugs) and pain medication. Meloxicam has been shown to be
safe over an extended period of time in rabbits,
with no reported side effects. The use of glucocorticosteroids in the treatment of ear infections
is a controversial topic. It is recommended to use them during the initial
days of treatment to reduce inflammation. However, caution should be
exercised to ensure their use does not exceed five days, as they possess immunodepressive properties. In the event
of otitis interna, it is advisable to administer meclizine, a drug
used to treat motion sickness. If the rabbit
has trouble eating and drinking, force-feeding and administration of SC
fluids are necessary. Damage to the
middle ear or nerves can result in irreversible hearing loss or head tilt. The prognosis
for surgical drainage procedures, such as bulla osteotomy, is unfavorable,
and these procedures often result in postoperative complications in rabbits.
This surgery is intended for use in cases of severe infection of the middle
or inner ear, when antibiotics prove ineffective in managing the condition.
Kei
Rivers Holly, the rabbit of Kei Rivers (New-Zealand). This video is a testimony that a rabbit suffering from head-tilt can continue to enjoy a good quality of life, without need to pts. Acknowledgement
My deepest gratitude to Dr. Zahi Aizenberg,
(The Koret School for Veterinary Studies, The Hebrew University of Jerusalem,
Bet-Dagan, Israel) and to Dr. Estella Böhmer (Chirurgische
u. Gynäkologische Kleintierklinik,
Ludwig-Maximilians-Universität München, Germany) for the permission to use
their pictures. Many
thanks also to Renee Brennan for sharing the video of her head-tilted rabbit
Rudy and to Kei Rivers for sharing her video of Holly. Further information
Bjotvedt G, Geib LW. Otitis media associated with Staphylococcus
epidermidis and Psoroptes cuniculi in a rabbit. Vet Med Small Anim
Clin. 1981; 76(7):1015-6. Flatt RE, Deyoung
DW, Hogle RM. Suppurative otitis media in the rabbit: prevalence, pathology,
and microbiology. Lab Anim Sci. 1977; 27(3):343-7. Fox RR, Norberg RF, Myers DD. The
relationship of Pasteurella multocida to otitis media in the domestic
rabbit (Oryctolagus cuniculus). Lab Anim Sci. 1971; 21(1):45-8. Harcourt-Brown F. Rabbit Medicine and
Surgery, Oxford, UK: Butterworth-Heinemann 2001, 192 pages. Hillyer EV, Quesenberry QE. Ferrets, Rabbits,
and Rodents: Clinical Medicine and Surgery New York: WB Saunders Co.,1997,
432 pages. Kunstyr I, Naumann S. Head tilt in rabbits caused by
pasteurellosis and encephalitozoonosis. Lab Anim.
1985; 19(3):208-13. Ladefoged O. The absorption half-life, volume
of distribution and elimination half-life of trimethoprim after peroral
administration to febrile rabbits. Zentralbl Veterinarmed A. 1979; 26(7):580-6. Murray KA, Hobbs BA, Griffith JW. Acute
meningoencephalomyelitis in a rabbit infected with Pasteurella multocida.
Lab Anim Sci. 1985; 35(2):169-71. Richardson V. Rabbits: Health, Husbandry and
Disease, Blackwell Science Inc, 2000, 178 pages. Snyder SB, Fox JG, Campbell LH, Soave OA.
Disseminated staphylococcal disease in laboratory rabbits (Oryctolagus
cuniculus). Lab Anim Sci. 1976; 26(1):86-8. Snyder SB, Fox JG, Soave OA. Subclinical otitis media associated with Pasteurella
multocida infections in New Zealand white rabbits (Oryctolagus
cuniculus). Lab Anim Sci. 1973; 23(2):270-2. |

e-mail: info@medirabbit.com
