![]()
Corneal
abrasion and ulceration in rabbits
Esther van Praag, Ph.D.
|
|
MediRabbit.com is
funded solely by the generosity of donors. Every
donation, no matter what the size, is appreciated and will aid in the
continuing research of medical care and health of rabbits. Thank you |

Warning: this file
contains pictures that may be distressing for people.
The cornea, or transparent front part of the eye, is a thin dense
fiber-like structure characterized by 4 distinctive layers in rabbits:
• A keratinized layer of epithelium (30 to 40
mm);
• The stroma, formed by parallel bundles of
collagen;
• The Descemet’s membrane (7 to 8 mm);
• A single layer of endothelium, which is
rich in Na+-ATPase pumps.
The cornea covers up to 30% of the rabbit eye. Due to its large size,
the cornea is prone to trauma or other damages, including drying-out. If the
epithelial layer of the cornea is scratched or wounded, it may become locally
opaque and neo-vascularization has been observed.
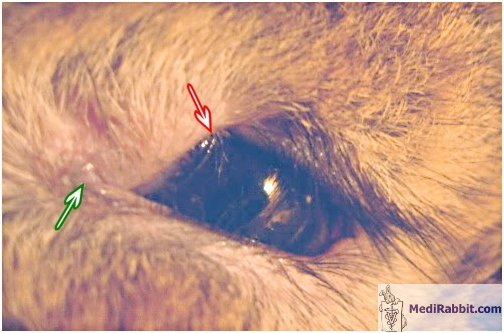
Damage and ulceration of the cornea are painful, as the surface of
the cornea is well innervated. As a result, a rabbit will rub the affected
eye, which can lead to the development of an ulcer, and keep the eye closed.
It is often accompanied by dacryocystitis. Contraction of the pupil,
conjunctival hyperemia (presence of excess blood), and epiphora (increased
production of tears) can furthermore be the result of pain caused by the
ulcer. The rabbit is depressed and can stop eating or drinking.
Causes
For an extended list of causes for keratitis, corneal damage and
ulceration, see: Corneal ulcers in
rabbits.
Diagnosis
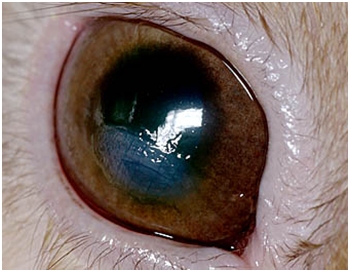
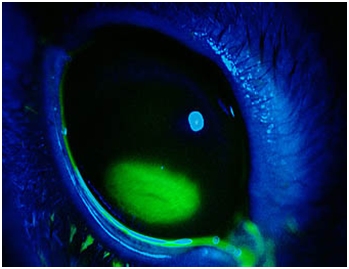
An opacity and/or inflammation on the surface of
the eye can be indicative of a superficial corneal abrasion. The use of a
fluorescent dye (fluorescein) helps determine the extent of the damage, and
its depth. It can be accompanied by a secondary bacterial infection (abscess,
uveitis).
If an infection is present, it is necessary to take
a sample for a bacterial culture and antibiotic sensitivity test, before the
application of the dye.
The size of a corneal ulcer varies and necrotic tissue may be
present. It may accompanied by a temporary constriction of the pupil
(miosis), or inflammation of the uvea (uveitis). In rare cases the ulcer becomes indolent,
without healing.
The presence of corneal damage may be accompanied by an overflow of
tears (epiphora), involuntary closing of the eyelids (blepharospasm),
accumulation of blood (conjunctival hyperemia) or secondary abscessation.
Underlying disorders or diseases should not be ruled out. Indeed,
corneal ulceration can be the result from exophthalmia (protruding eyeball),
leading to the impossibility to blink, the presence of a retrobulbar abscess,
neoplasia, cellulitis, or tooth root related problems, like the presence of
an abscess or abnormal elongation of the tooth root in the direction of the
eye socket. Abnormal growth of the eyelashes (e.g. entropion, distichiasis)
is a further cause for corneal abrasion and ulceration.
Treatment
The treatment depends on the type of ulceration (abrasion, ulcer or
descemetocele) as well as the cause, if it is superficial or deep, and its
extent.
The treatment of superficial abrasion and ulcers includes the
application of a topical antibiotic solution 4 to 6 times a day. Their effect
may last a few minutes only in rabbits. Topical atropine has good healing
properties and needs to be given twice a day only. The treatment should be
accompanied by the administration of analgesics. Healing is usually observed within 3 to 5
days.
In the case of a corneal ulcer or descemetocele, the eye must be
protected. The treatment should be aggressive, with frequent application of
topical antibiotics (e.g. ciprofloxacin 3%, ofloxacin 0,3%, norfloxacin 0,3%
are antibiotics of choice) and the use of pain relief medication (e.g.
meloxicam).
Persistant
non-healing corneal ulcers are characterized by the accumulation of dead
cells at the edge of the ulcer, which will prevent healing. In this case, the
area must be debrided, so that cells from the healthy corneal surface can
start migrate towards the ulcer and fill the gap. A local or full anesthesia
is necesary before corneal debridement can be started with e.g., a dry
cotton-tipped applicator. Grid keratotomy,
superficial keratotomy or the placement of contact-lenses have also been used
to cure non-healing ulcers in rabbits. When the abrasion or the ulcer is related to underlying
anatomical or pathological causes (e.g., abscess, dacryocystitis, blepharo-
or keratoconjunctivitis), these must be treated or corrected too, either
medically or surgically (e.g. entropion, distiachiasis). Acknowledgement
Thanks are due to Ivy (Serbia), to Amy Carpenter (USA) and Akira
Yamanouchi (Veterinary Exotic Information Network, https://vein.ne.jp/, Japan), for the
permission to use their pictures. Thanks
also to Grijsje.
Further
information
Andrew SE. Corneal
diseases of rabbits. Vet Clin North Am Exot Anim Pract. 2002; 5:341-56.
Review.
Flecknell P., editor
Gloucester, BSAVA Manual of Rabbit Medicine and Surgery, UK: British Small
Animal Veterinary Association2000.
Hillyer E.V. and
Quesenberry K.E., Ferrets, Rabbits, and Rodents: Clinical Medicine and
Surgery, New York: WB Saunders Co. 1997.
Fox JG, Shalev M,
Beaucage CM, Smith M. Congenital entropion in a litter of rabbits. Lab Anim
Sci. 1979; 29:509-11.
Kern T.J., Ocular
disorders of rabbits, rodents and ferrets. In: Kirk R.W., Bonagura J.D., eds.
Current veterinary therapy X.
Philadelphia, WB Saunders, 1989.
Manning P.J.,
Ringler D.H., Newcomer C.E. The Biology of the
Laboratory Rabbit, New York: Academic Press1994.
Okerman, L:
Diseases of Domestic Rabbits, 2nd Edition, Blackwell Scientific Publications,
London, 1996.
|
|||||||||




e-mail: info@medirabbit.com
