|

Warning: this page contains pictures that may be distressing for some
persons.
|
Corneal ulcer
|
|
|
Well it looks like an ulcer with purulent inflammatory
material at its lower edge doesn't it? But the cornea was fluorescein-negative
and here's the other eye! No money for cytology and bacteriology so its on
topical antibiotic and NSAID and I'll let you know what happens. Don't
always expect me to have the answer straight away!
(c)
2006 Dr David L Williams
|
|
Cataract
|
|
|
If
this were a dog we would say for sure it was a diabetic catarct, given its
mature appearance and rapid onset. But in a rabbit things aren't quite so
simple; the animal has no other signs of diabetes and most importantly the other
eye still has a clear lens! Not all diagnoses are as straight forward as we
would like them to be! More importantly the animal is behaviourally
unaffected and needs no treatment. It is always possible that
Encephalitozoan cuniculi is involved in cataractogenesis here, but here the
owner was not concerned enough to warrant serological confirmation of this.
(c)
2005 Dr David L Williams
|
|
Keratitis and Wessely ring
|
|

|
photograph
(c) 2005 Alice Courtney text (c) 2005 David Williams
|
|
Retrobulbar abscess
|
|
|
This is exophthalmos caused by a retrobulbar space occupying mass. It could
be a tumour or an abscess, but in a rabbit that latter is far more likely.
Here is an MRI of the head, showing pus extending up in the orbit and then
down as far as the cervical area. The kindest thing in this case was
euthanasia. Less severe lesions could be treated with enucleation and
orbital exenteration, but even then the infection almost always recurs at
some point.
(c)
2005 Dr David L Williams
|
|
Dacryocystitis
|
|
|
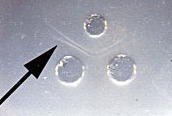
This is dacryocystitis -
inflammation (and in all probability infection) or the nasolacrimal duct.
The rabbit has a narrow duct with two points at which the duct bends and
narrows. This, together with the likelihood of maxilary bone involvement in
nutritional bone disease and dental abnormalities, leads to this build up a
pus, shown well here as it leaves the single nasolacrimal punctum. Regular
flushing and probably systemic antibiotic therapy too are steps to
resolutin of the problem, but the road to a cure, like the nasolacrimal
duct iteslf, is long and tortuous!!
(c) 2005 Dr David L Williams
|
|
|
|

|
Here the intraocular pressures were
45mmHg in each eye and the condition was glaucoma caused by the bu gene.
Other possibilities might include retrobulbar abscessation, although this
would be rare bilaterally, and venous congestion causing retrobulbar plexus
engorgement, again a very rare condition. The bu gene is common in New
Zealand White rabbits like this one, causing a dysplastic iridocorneal
angle where drainage is very poor. A useful paper on the condition is Ueno
and colleagues report on Histopathological changes in iridocorneal angle of
inherited glaucoma in rabbits. Graefes Arch Clin Exp Ophthalmol.
1999;237:654-60
(c) 2005 Dr David L
Williams
|
|
|
|


|
While such masses could
be inflammation or tumour of many different sorts, the vast majority in
domestic rabbits are associated with myxomatosis. The relation between the
myxoma virus and the host rabbit is a fascinating story (very well reviewed
in Zuniga MC: A pox on thee! Manipulation of the host immune system by
myxoma virus and implications for viral-host co-adaptation. Virus Res. 2002
88:17-33) with viral virulence factors and host resistance in a major
host-virus battle. This rabbit had been vaccinated and thus was not as
severely affected as an unvaccinated animal such as this poor rabbit.
(c)
2004 Dr David L Williams
|
|
|
|
|
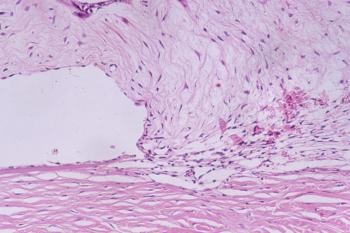
The
dense white mass lesion in the iris with vascularisation is virtually
pathognomonic for a lens-induced uveitis associated with Encephalitozoan
cuniculi infection. The pathogenesis appears to be that the parasite
enters the lens in utero and exits later sometimes giving cataract and
sometimes a lens-induced inflammation, characteristically appearing as a
variably vascularised white mass. Treatment can be by phacoemulsification
of the lens, but a medical therapy if surgery is not possible, involves
anti-inflammatory medication with topical steroid or NSAID and
anti-parasitic systemic medication such as oral albendazole.
(c)
2004 Dr David L Williams
|
|