![]()
Cardiology and Techniques for
Detecting Cardiac Diseases
in Rabbits
Esther van Praag Ph.D.
|
|
MediRabbit.com is funded solely by the generosity of
donors. Every donation, no matter what the
size, is appreciated and will aid in the continuing research of medical care
and health of rabbits.
Thank
you |

Warning: this page contains pictures that may be distressing for some persons.
Cardiology in pet rabbits is a
domain in which the amount of available information is limited. Therefore,
the incidence of cardiac problems is not well documented.
Despite the paucity of
information, a complete cardiac study—including radiography,
electrocardiography, and/or ultrasound analysis—can be used to diagnose the
problem and treat the cardiac disorder appropriately.
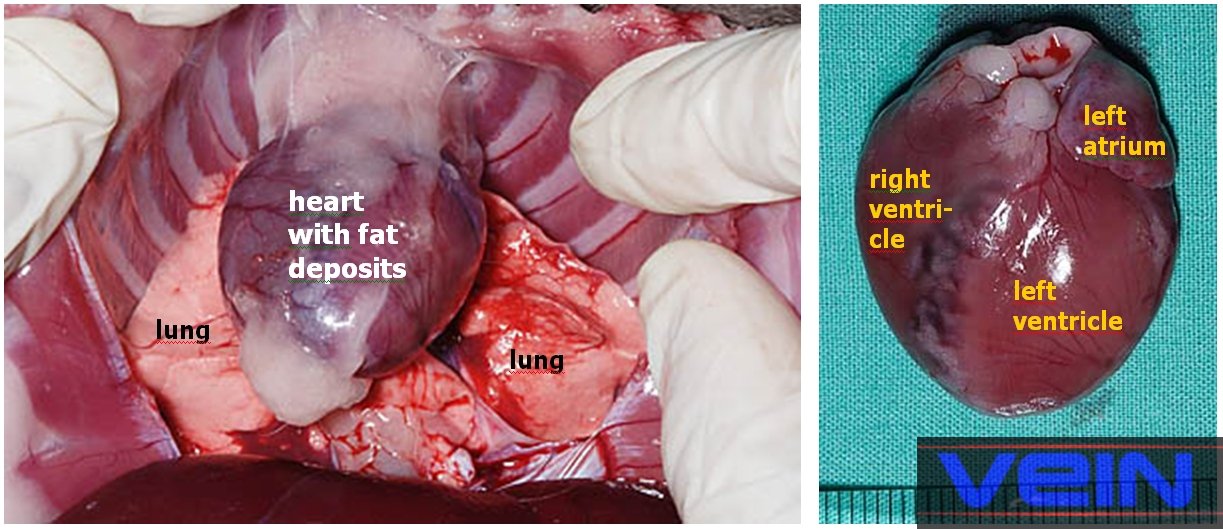
The
heart is located in the thoracic cavity, with the
apex (tip of the heart) directed backward and slightly to the left; the base
is directed forward. As observed in other small animals, the rabbit heart has
four chambers: The heart is composed of two auricles and two ventricles,
which are separated by inter-auricular and inter-ventricular septa.
Additionally, it exhibits certain anatomical particularities:
• The right
and left ventricles constitute the muscular caudal portion of the rabbit
heart. The left ventricle is larger than the right one, and the
interventricular septum separates them. Their walls are raised into muscular
ridges. The right ventricle is significantly thicker than the right auricle
and forms the right side of the conical apical portion, though it does not
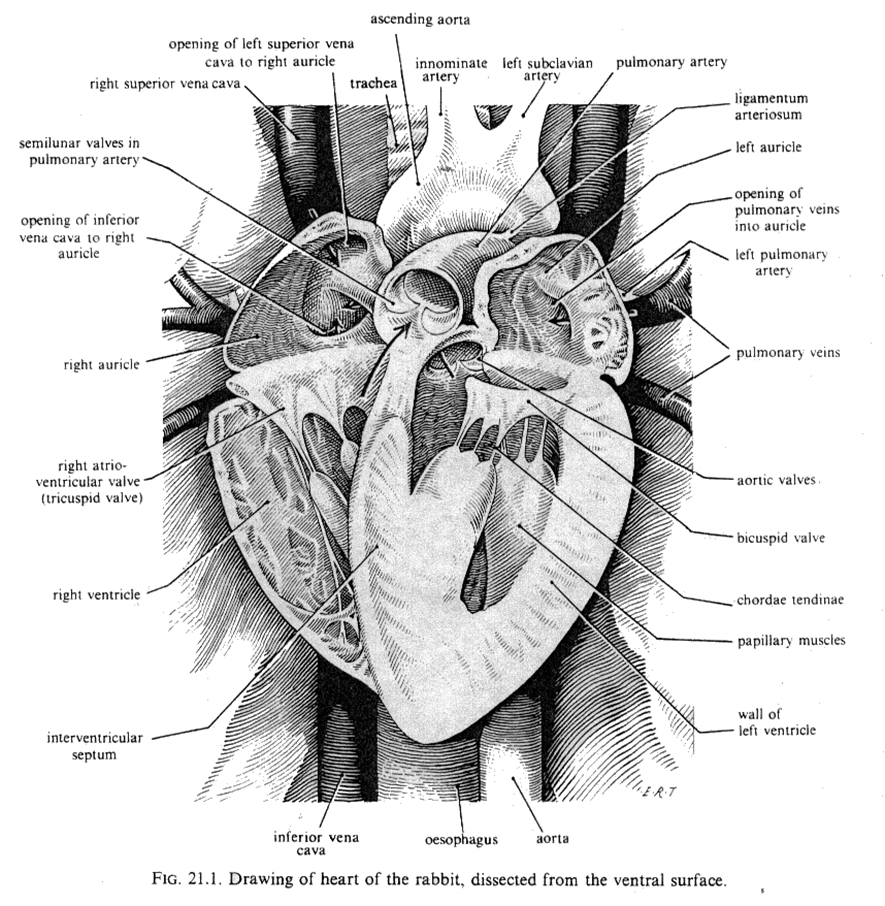
extend to the apex. It gives off the pulmonary artery in the anterior
position. Cusp valves separate the ventricular chambers from the pulmonary
artery and the aorta.
The
ventricular chambers are separated from the auricles by flap valves, which
are held in place by tendons. The tricuspid valve, which connects the right
auricle and right ventricle, has two cusps rather than three, which is
typically observed in other animals.
• The right
and left auricles are located in the cranial part of
the heart. These chambers receive the venous blood from:
• The
cranial and caudal vena cava (one of two large veins that return blood from
the body's outer parts to the right chamber of the heart) and the coronary
sinus (which receives blood from the heart itself) are drained into the right
auricle,
• The left
and right pulmonary veins, which carry oxygenated blood from the lungs, open
into the cavity on the dorsal side of the left auricle. Each auricle
possesses, in addition, small muscular flaps.
The
sinoatrial node, also known as the pacemaker that initiates the heartbeat, is
found in the right atrium.
The
rabbit heart exhibits distinct physiological characteristics that set it
apart from the hearts of other small animals:
• The
aortic nerve contains baroreceptors but lacks chemoreceptors. This indicates
that it does not possess sensory nerve cells that are activated by chemicals;
rather, it has only pressure-sensitive nerve endings. These nerve endings
stimulate reflex mechanisms that allow the body to adapt to changes in blood
pressure by dilating or constricting the blood vessels.
• The
pulmonary artery and its branches are composed of highly developed muscular
tissue.
• The
coronary arteries, which supply the cardiac muscle and originate from the
aorta, are susceptible to compression, potentially resulting in myocardial
ischemia due to poor collateral circulation.
Rabbit cardiac
parameters
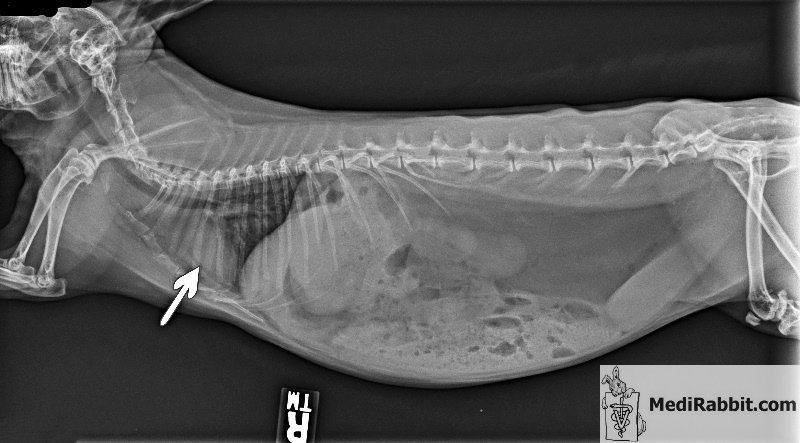
Rabbit abdominal
radiography
An X-ray of the rabbit's
abdominal region is a standard diagnostic procedure in cases of dyspnea
(shortness of breath), persistent cough, chest injury, or suspected
pneumonia. The results will include detailed information regarding the shape
and size of the heart and lungs. It can detect heart failure, emphysema, the
possible presence of pulmonary edema, the vascular pattern, the presence of
abscesses or neoplasia (e.g., thymoma, lung cancer), and other medical
conditions. However, it is important to note that this technique is not
without its limitations. Small malignant tumors can be too small to be
visible. Pulmonary embolism, or blood clots in the lungs, is not observed
either, and further study is required.
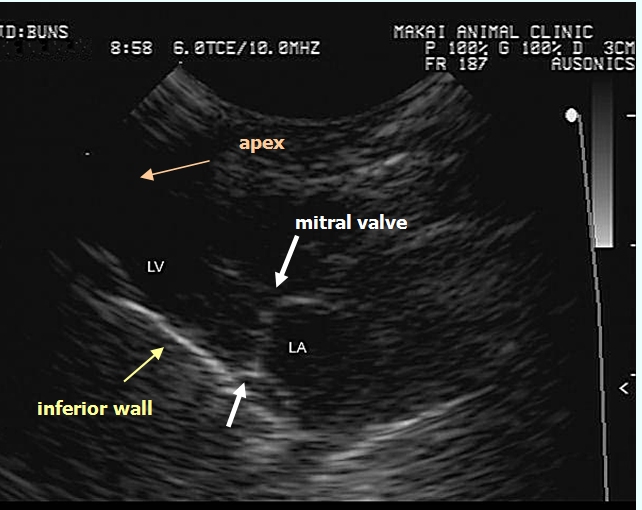
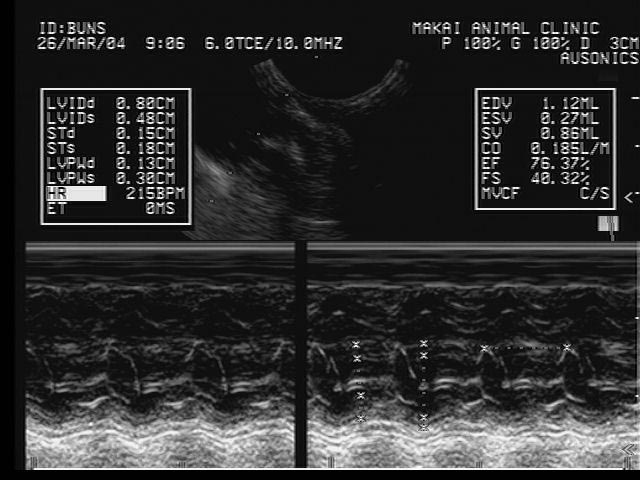
Rabbit ultrasound
examination or echocardiography
Most rabbits tolerate the
harmless, non-invasive, and widely available method of echocardiography
without the use of sedative drugs, which can modify the heart
characteristics. The method is characterized by its sensitivity and
precision, ensuring the capture of high-quality images. Given the rapid
heartbeat of rabbits and the small size of their hearts, it is necessary to
use equipment with a high-frequency transducer (handheld recording probe) and
a high-frame-rate ultrasound machine. Echocardiography is used to
detect abnormalities in the structure of the heart, including defective heart
valves and congenital defects. It also allows for the assessment of heart
wall or chamber enlargement, such as in cases of heart failure or cardiomyopathy.
Additionally, echocardiography provides information about heart wall motion
and the volume of blood pumped from the heart with each heartbeat. It can
also identify the accumulation of fluids in the pericardium (pericardial
effusion) or the presence of scar tissue throughout the pericardium. Specialized techniques, such as
M- or TM-mode (M = movement, T = time) ultrasound, will provide valuable
information for analyzing wall and valve movements. The B-mode technique (B =
brightness) is used to examine anatomical relationships (e.g., heart structure,
valves). Color Doppler ultrasonography is used to determine the direction of
blood flow and/or its velocity. It can thus detect turbulent flow due to
narrowing or blockage of blood vessels.
Rabbit
electrocardiography (ECG or EKG)
Electrocardiography (ECG) is a
commonly used, non-invasive, simple, and painless procedure that enables the
recording of electrical changes in the heart by amplifying electrical
impulses that flow through the heart. Electrocardiography is used to evaluate
and manage a wide range of cardiac-related symptoms, including chest pain,
dyspnea, palpitations, arrhythmias, and syncope. The rhythm in a healthy rabbit
shows a sine wave. It excludes respiratory sinus arrhythmia (RSA) because the
flow of sympathetic and vagus impulses to the
sinoatrial node is not influenced by breathing. The electrocardiogram (ECG)
provides a series of waveforms that offer valuable insights into various
aspects of the cardiac system. Specifically, it reveals information about the
pacemaker (that triggers each heartbeat), the nerve conduction pathways of the
heart, and the heart's rate and rhythm. The waves are designated P, Q, R, S,
and T in alphabetical order: • P
wave of the electrocardiogram is associated with the atrial contraction, • QRS
series of waves is associated with ventricular contraction, • P-Q
or P-R interval gives a value for the time taken for the electrical impulse
to travel from the auricle to the ventricle. • T
wave comes after the contraction. Electrocardiogram values for a
healthy rabbit:
Variation
is the values presented in the above table may indicate: • Abnormal P wave: right or left atrial
hypertrophy, atrial premature beat, hyperkalemia. • Abnormal QRS interval: right or left
bundle branch block, ventricular rhythm, hyperkalemia, among others. • Abnormal Q-T duration: hypocalcemia,
hypothyroidism, brain hemorrhages, congenital deformations, myocardial
infarction, myocarditis. • Abnormal T wave: hyperkalemia, hyperacute
myocardial infarction and left bundle branch block in case of a tall T wave;
ischemia, age, stress, pericarditis, intraventricular conduction delay,
electrolyte disturbance, in case of a small, flattened or inverted T wave. Rabbit cardiac disorders
A variety of medical conditions
have been identified in rabbits, including congestive heart failure, cardiac
myopathy (e.g., myocardial fibrosis), and congenital heart diseases (e.g. atrial
or ventricular septal defects, arrhythmia, valvular diseases, or vascular
diseases). Acknowledgement I would like to
express our gratitude to Tom Chlebecek, DVM, (Makai Animal Clinic, Kailua,
HI), Frossie Economou, Kim Chilson, and Akira
Yamanouchi, (Veterinary Exotic Information Network, https://vein.ne.jp/), for
their kind permission to use the pictures. I would also like to express my
gratitude to Dr. Tom Chlebecek for his comments. Further
information M.V. Bray MV, WE. C. Weir EC, D. G. Brownstein, M.
L. Delano, (1992) Endometrial venous aneurysms in three New Zealand white
rabbits. Lab Anim Sci.; 42(4):360-2. Farkas, A. J. Batey, S. J. Coker (2004) How to
measure electrocardiographic QT interval in the anaesthetized rabbit. J Pharmacol Toxicol Methods.;
50(3):175-85. L.C. St John, F. P. Bell (1990) Arterial fatty
acid-binding protein activity associated with dietarily-induced and
spontaneously occurring atherosclerosis in the rabbit (Oryctolagus
cuniculus). Comp Biochem Physiol
B.; 97(1):123-7. C. Kozma, W. Macklin, L. M. Cummins, R. Mauer
(1974) The anatomy, physiology and biochemistry of the rabbit, in The Biology
of the Laboratory Rabbit (Weisbroth et al., eds),
pp 50-69. L. I. Kupferwasser, M.
R. Yeaman, S. M. Shapiro, C. C. Nast, A. S. Bayer (2002) In vitro
susceptibility to thrombin-induced platelet microbicidal protein is
associated with reduced disease progression and complication rates in
experimental Staphylococcus aureus endocarditis: microbiological,
histopathologic, and echocardiographic analyses. Circulation; 105(6):746-52. C. J. Orcutt (2000) Cardiac and respiratory
disease in rabbits. Proceedings of the British veterinary Zoological Society
(Autumn meeting) K. E. Quesenberry, J. W. Carpenter, P. Quesenberry
(2004) Ferrets, Rabbits and Rodents: Clinical Medicine and Surgery Includes
Sugar Gliders and Hedgehogs, Elsevier Health, pp 211-216 R. S. Simons (1996) Lung morphology of cursorial
and non-cursorial mammals: lagomorphs as a case study for a pneumatic
stabilization hypothesis. J Morphol. 1996; 230(3):299-316. F.
Harcourt-Brown, Textbook of Rabbit Medicine, UK: Butterworth-Heinemann, 2001. |

e-mail: info@medirabbit.com
